October 4th, 2009 by DrWes in Better Health Network, True Stories
No Comments »

It was midnight and the Emergency Room door opened like a curtain on a Broadway. A lone man sat in blue at the countertop, writing. Behind him, the chorus, working feverishly on the protagonist – the script rehearsed a thousand times before.
Clothes off, Story?, facemask, C-collar, endotracheal tube, breath sounds, telemetry, IV’s, blood work, pulse ox, Stop.
Resume, Pulse?, patches, register, call the lab, Allergies?, epi, atropine, Pressure?, twitching, NG, x-ray, Stop. Pulse?
Resume, pacing wire, max output, capture?, not quite, “potassium?”, not ready, blood gas, foley, Capture! Stop.
Resume, blood gas, no capture, damn, tweak, better, pulse?, yes. Lab?, no, Which meds?, cardiologist, Go.
Vent, hoist, prep, stick, contrast, open, shock, balloon pump, a-line, movement, labs, blood gas, peep, transport, c-spine, CT, Go.
Then intermission. Read more »
*This blog post was originally published at Dr. Wes*
September 30th, 2009 by DrWes in Better Health Network, Health Policy, Opinion
No Comments »
It’s the holy grail of physician payment reform: ending fee-for-service payments to doctors and, instead, pay doctors based on the quality of care they perform. Remarkably, Congress feels they’ve found the answer:
Thus, the new language in the Senate Finance bill would finally connect Medicare reimbursements to quality, as opposed to volume.
The measure gives the secretary of Health and Human Services, working with the Centers for Medicare and Medicaid Services, the power to develop quality measurements and a payment structure that would be based on quality of care relative to the cost of care. The secretary would have to account for variables that include geographic variations, demographic characteristics of a region, and the baseline health status of a given provider’s Medicare beneficiaries.
The secretary would also be required to account for special conditions of providers in rural and underserved communities.
Additionally, the quality assessments would be done on a group-practice level, as opposed to a statewide level. Thus, the amendment would reward physicians who deliver quality health care even if they are in a relatively low quality region.
The secretary of Health and Human Services would begin to implement the new payment structure in 2015. By 2017, all physician payments would need to be based on quality.
Wow. That sounds great! But there’s just one problem…
… how do we define “quality?”
Read more »
*This blog post was originally published at Dr. Wes*
September 21st, 2009 by DrWes in Better Health Network, Opinion
No Comments »
Here’s a dumb thought: If you want to save costs on medical devices to the federal government, require a tax fee concessions of $4 billion dollars from the medical device companies to fund a health care overhaul.
Now either that $4 billion will get added to the cost of devices (and the patient/insurer’s tab) or the device companies will decide that they must pay the fee to maintain their current pricing.
Government pressures hospitals and doctors by paying less, so hospitals keep the heat on medical device makers to lower costs so they can make their margins.
It all sounds good, right?
But according to one analyst, it seems device makers would rather pay the fee than make their prices transparent:
But the mechanism for how devices companies might pay matters more than what they pay, according to Morgan Stanley analyst David Lewis. “A ‘flat tax’ is preferable, in our view, to targeted industry fees as our larger concern is the creation of more infrastructure intended to catalyze pricing transparency,” he said.
And so, with the fee, the government pays itself while the medical device prices continue to remain inflated.
Why do the patients always seem to lose with these government-mandated scenarios?
-Wes
*This blog post was originally published at Dr. Wes*
September 16th, 2009 by DrWes in Better Health Network, Opinion
No Comments »
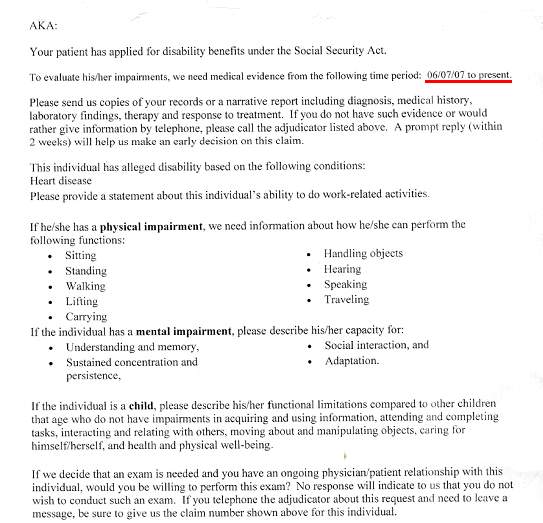
This week, like many doctors in primary care, I was sent a request by the Social Security to provide “medical evidence” that one of my patients was disabled so they could collect Social Security benefits. As part of that request, I was asked to provide evidence since June 6th, 2007, that my patient qualified for disability on the basis of “alleged” diagnosis of “Heart Disease.”
I was asked to send “copies of records or a narrative report including diagnosis, medical history, laboratory findings, treatment and response to treatment.” Beyond this, I also had to include physical and emotional impairment assessments and a functional assessment of their ability to sit, stand, walk, lift carry, handle objects, hear, speak, travel, and wash their car, view films, and eat bon bons (well, kind of).
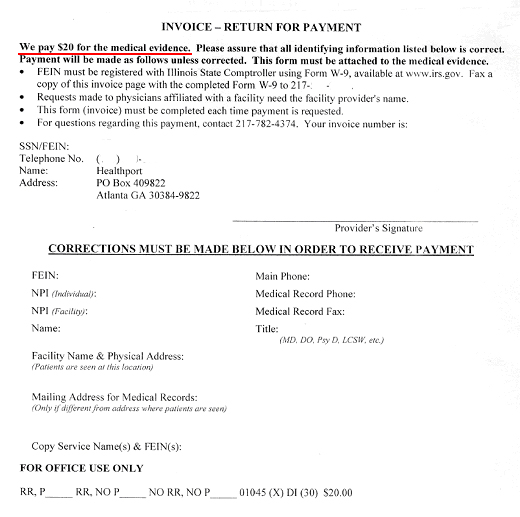
And for this copying, writing, mailing, collating what might I see from the government to compensate my time? Well, if I attach this invoice that requires a Federal Employee Identification Number filed through form W-9 available at www.irs.gov (yes, Virginia, this compensation is taxed), I might receive…
…drum roll, please…
… twenty dollars.
Now looking up the lowest paygrade of Social Security worker’s annual compensation of $29,726 and accounting for the 13 vacation days, 13 paid sick leave days, and 10 federal holidays they get paid, I estimate the least expensive Social Security employee makes a bit more than $16.50 an hour.
If we assume that the paperwork they just asked for takes about 2 hours collectively of office staff and doctor time, I think it’s clear that doctors’ payment for this service provided on behalf of our patients is substantially less than what the Social Security administration pays their own staff.
I wonder what else the government has in store for us.
-Wes
*This blog post was originally published at Dr. Wes*
September 7th, 2009 by DrWes in Better Health Network, Health Policy, Health Tips
No Comments »
“I don’t know what could be more clear,” said Representative Bruce Braley, Democrat of Iowa, who has read aloud from a section of the House bill with the title “No Federal Payments for Undocumented Aliens.”
“Heath Care Debate Revives Immigration Battle,”
New York Times, 6 Sep 2009
From House Bill 3200, page 143:
SEC. 246. NO FEDERAL PAYMENT FOR UNDOCUMENTED
4 ALIENS.
5 Nothing in this subtitle shall allow Federal payments
6 for affordability credits on behalf of individuals who are
7 not lawfully present in the United States.
* * *
Taxpayers are concerned whether they will have to foot the bill for illegal aliens in the upcoming health care bill. Many ask good questions, like how will health care workers know who’s an illegal alien? If they are included, how will it be paid for? These are important questions that we would hope could be dealt with squarely, openly and with full transparency.
But this is a sensitive topic for Congressmen interested in securing reelection.
During the summer recess, many Congressmen were barraged by questions to this effect. So it was interesting reading this New York Times piece this morning on whether illegal aliens will be covered under the new health care plan before Congress. On one hand we have Congressmen placating his constituents by assuring voters that “I don’t know how it could be more clear” as they suggest taxpayers will not fund illegal aliens, but careful inspection discloses that illegal aliens will just not be eligible for federal subsidies to reduce their payments for federally-supplied health insurance.
But from here, it gets even more byzantine:
… the report finds that the House bill would not prohibit illegal immigrants from enrolling in a health insurance exchange. The exchange would allow participants to buy coverage from one of several plans, including a public option offered by the federal government.
At the same time, illegal immigrants would not be exempt from the obligations in the House bill. According to the research service, most illegal immigrants in the country would be required to buy health insurance or face tax penalties.
And since they would be barred from subsidies, they would have to pay for coverage at full rates, regardless of their income level.
So here we have illegal aliens, already strapped for cash, paying their “full payment” and if they don’t, the tax man will come after them (which is confusing to me, because I didn’t know that illegal aliens pay taxes).
So what is wrong with the public? How could they possibly be confused?
Here’s a thought: the only real way out of these shameful machinations is to deal with the immigration and health care issue separately, incrementally, and without this shell game. Doesn’t the American public deserve a more thorough discussion of this issue, rather than shoving it in to our upcoming health care legislation?
My personal sense of it is that such an issue will never be decided at the Emergency Room door. Rather, it is part of a systemic immigration control and reform question that involves our borders, employee verification, and a decision about existing illegal immigrants.
What we’re observing instead, is a Congress is too scared to deal with this issue honestly.
*This blog post was originally published at Dr. Wes*









{kind=link}
{kind=link}