September 16th, 2009 by RamonaBatesMD in Better Health Network, Health Tips
No Comments »

I’m sure I don’t see as many patients with common skin warts as my family practice or dermatology colleagues, but these patients still make it to my office. Sometimes it’s the primary complaint, sometimes it’s an afterthought. In reviewing the topic, it occurred to me that most patients don’t need to see any of us for this problem. They mostly need to accept the fact that the treatment takes TIME. So if you will persist, then you will often be successful without the expense of seeing a doctor. (photo credit)
Common warts (Verruca vulgaris) are caused by the human papillomavirus (HPV). Warts on the hands or feet do not carry the same clinical consequences of HPV infection in the genital area. It is estimated about 10% of children and adolescents have warts at any given time. As many as 22% of children will contract warts during childhood.
Common warts can occur anywhere on the body, but 70% occur on the hand. Often they will disappear on their own within a year. Even with treatment, warts can take up to a year to go away.
Before heading to the doctor, there are treatments you can try at home: salicylic acid or duct tape.
When using the 17% salicylic acid gel (one brand name: Compound W), it must be applied every day until the wart is gone. Only apply to the wart, not the skin around the wart. This treatment is enhanced by covering the wart with an occlusive water-proof band-aid or duct tape after applying the acid. It can also be enhanced by gently filing the wart with an emery board daily to remove the dead cells prior to applying the salicylic acid. Treatment can take weeks to months. Don’t give up early.
Duct Tape can take weeks or months to be effective. Apply the duct tape to the wart and keep it in place for six days. After removing the tape, soak the wart, and pare it down with a filing (emery) board. Repeat the above until the wart disappears. Once again, don’t give up early.
The two treatments (salicylic acid and duct tape) can be combined. Apply the salicylic acid liquid to the wart before bedtime. After letting it air dry for a minute or so, then apply the duct tape over the wart, completely covering the area. Remove the duct tape the following morning. Each time you remove the tape, you will be debriding some of the wart tissue. Repeat the application each night, until there is no remaining wart tissue. As with using only one treatment, don’t give up early.
If the above don’t work or you just don’t want to take the time, then you may wish to see your physician for removal. He can use cryotherapy to destroy the wart. This method may involve repeated treatment over several weeks. You can do the following to “get the wart ready for removal” and make the cryotherapy more effective:
-
Every night for 2 weeks, clean the wart with soap and water and put 17% salicylic acid gel (one brand name: Compound W) on it.
-
After putting on the gel, cover the wart with a piece of 40% salicylic acid pad (one brand name: Mediplast). Cut the pad so that it is a little bit bigger than the wart. The pad has a sticky backing that will help it stay on the wart.
-
Leave the pad on the wart for 24 hours. If the area becomes very sore or red, stop using the gel and pad and call your doctor’s office.
-
After you take the pad off, clean the area with soap and water, put more gel on the wart and put on another pad. If you are very active during the day and the pad moves off the wart, you can leave the area uncovered during the day and only wear the pad at night.
If none of the above work, then your wart may need to be removed surgically. Remember the above all take time, so give them time to work. Even if the wart disappears with any of the above treatments, it may recur later.
Sources
Treatment of Warts; Medscape Article, May 27, 2005: W. Steven Pray, PhD, DPh; Joshua J. Pray, PharmD
What Can Be Done About a Hand Wart That Keeps Reappearing After Removal?; Medscape Article, May 31, 2007; Richard S. Ferri, PhD, ANP, ACRN, FAAN
Duct tape and moleskin equally effective in treating common warts; Medscape Article 2007; Barclay L.
Duct Tape More Effective than Cryotherapy for Warts; AAFP, Feb 1, 2003; Karl E. Miller, M.D.
*This blog post was originally published at Suture for a Living*
September 16th, 2009 by DrRob in Better Health Network, Health Policy
No Comments »

I got something in my e-mail this morning. It’s a press release aimed at helping with prostate cancer awareness month, and is supported by Lance Armstrong’s foundation.
SURVEY SHOWS AT-RISK MEN LACKING IN PROSTATE CANCER KNOWLEDGE
SUNNYVALE, CALIF.,– September 9, 2009 – Prostate cancer remains one of the most commonly diagnosed cancers in the United States. In fact, one in six men will develop prostate cancer. It is also the second-leading cause of cancer death in the United States. But a recent survey suggests that many men at risk for the cancer still aren’t aware of all available treatment options. The survey, conducted late last year, reveals that nearly 50% of men aged 40 and older are not aware of the most common approach to surgery for prostate cancer — robotic-assisted surgery to remove the prostate. “I had to do my own research and then self-admit myself to the [hospital],” says surgery patient Tim Propheter. “…. Most people are just told … ‘Sorry, you have to have surgery, and we’ll set you up for such and such day,’ and they don’t know any better until they run into someone like me,” he says. This lack of information persists despite the fact that prostate cancer treatment has changed dramatically in the last decade. For example, surgery — which remains the gold standard treatment for localized prostate cancer — has become much less invasive. According to the American Urologic Association, the major benefit of prostatectomy, or prostate removal, is a potential “cancer cure” in patients with localized or early stage cancer.
Guess who the press release was from? Guess who sponsored the survey? The following was at the bottom of the email:
About the survey
Data was collected from 1000 self-selected adult healthcare information seekers through an online panel available through Ztelligence.com, using an survey questionnaire. Fifty-four percent of those were male and 46 percent were female. The results reflect only the opinions of the healthcare seekers who chose to participate.
About Intuitive Surgical, Inc.
The survey was conducted by Intuitive Surgical, Inc. (NASDAQ: ISRG), the manufacturer of the da Vinci Surgical System, the world’s only commercially available system designed to allow physicians to provide a minimally invasive option for complex surgeries. Intuitive Surgical, headquartered in Sunnyvale, California, is the global technology leader in robotic-assisted, minimally invasive surgery (MIS). Intuitive Surgical develops, manufactures and markets robotic technologies designed to improve clinical outcomes and help patients return more quickly to active and productive lives. The company’s mission is to extend the benefits of minimally invasive surgery to the broadest possible base of patients. Intuitive Surgical — Taking surgery beyond the limits of the human hand.™
Imagine that. A survey done by company that sells the da Vinci robotic surgical equipment shows that men have tragically no knowledge of the da Vinci robotic prostate surgery!
So let’s see what the evidence shows:
- Prostate cancer occurs in 186,000 men each year and kills nearly 29,000.
- In a well-known autopsy survey, over 1/3 of men over 80 were found to have cancer present in their prostate without evidence of significant disease. It is not clear how many of these men will progress to overt cancer, but it is very clear that this is the vast minority.
- PSA Testing (the blood test for prostate cancer screening) is by far the largest source of surgical candidates. It is a controversial test, having a high rate of false positives and an unproven record of significant benefit.
From the reference uptodate.com:
The European Randomized Study of Screening for Prostate Cancer (ERSPC) reported a small absolute survival benefit with PSA screening after nine years of follow-up; however, 48 additional patients would need aggressive treatment to prevent one prostate cancer death. Although the report did not address quality of life outcomes, considerable data show the potential harms from aggressive treatments. Further sustaining the uncertainty surrounding screening, a report from the large United States trial, the Prostate, Lung, Colorectal, and Ovarian (PLCO) Cancer Screening Trial, published concurrently with the European trial, found no benefit for annual PSA and digital rectal examination (DRE) screening after seven to ten years of follow-up. The crux of this screening dilemma was aptly stated by the urologist Willet Whitmore, who asked “is cure possible in those for whom it is necessary, and is cure necessary in those for whom it is possible?”
The most important line in this is at the end of the first sentence, stating that 48 patients would need aggressive treatment (including prostatectomy) to prevent one prostate cancer death. So how much does “aggressive treatment to prevent cancer death” cost?
From the Journal of Clinical Oncology:
For patients in the treatment-received analysis, the average costs were significantly different; $14,048 (95% confidence interval [CI], $13,765 to $14,330) for radiation therapy and $17,226 (95% CI, $16,891 to $17,560) for radical prostatectomy (P < .001). The average costs for patients in the intent-to-treat analysis were also significantly less for radiation therapy patients ($14,048; 95% CI, $13,765 to $14,330) than for those who underwent radical prostatectomy ($17,516; 95% CI, $17,195 to $17,837; P < .001).
note: it was very hard to find numbers here. This is actually from Medicare claims from 1992 and 1993, so it is a huge underestimate from today’s numbers.
Which means that based on the 1992 numbers, you would spend $672,000 to save one life using radiation therapy and $1,084,000 if you used surgery. This does not take into account the consequences of surgery for the men who underwent the surgery.
What about robotic surgery? In a comparison of the cost of open prostatectomy to robot-assisted surgery, the cost is even higher.
Cost was the one area in which the older open surgery was the clear winner: Open radical prostatectomy costs $487 less a case than non-robotic laparoscopy and $1,726 less than robot-assisted prostatectomy.
According to the review, “Shorter operative time and decreased hospital stays associated with the robotic procedure did not make up for the cost of the additional equipment expenditure.” Estimated costs of the robotic system to a provider run about $1.2 million a year, with maintenance costs of $120,000 a year and one-time costs of $1,500 a case.
To summarize:
- Prostate cancer screening is controversial, as it fails to differentiate between the minority of men who would die from the disease from the majority who would simply die with it.
- PSA Testing as greatly increased the number of men diagnosed with early stage cancers.
- Prostate cancer surgery or radiation therapy is recommended for men who have early stage cancers.
- Aggressive prostate cancer treatment has to be done 48 times to save one life.
- The most expensive treatment for prostate cancer is prostatectomy, or removal of the prostate.
- The robotic form of the surgery is a higher-cost procedure by a significant amount.
So, an expensive form of surgery that may not be appropriate is done on a group of men identified on a very unreliable test yielding a very small number of lives saved and a lot of men who then have to deal with the physical consequences of the surgery. Why in the world is this being promoted at all?
Money. Here’s the homepage of one of our local hospitals. They have aggressively marketed da Vinci surgery on television, billboards, and the radio.

Why do you think they would pay as much money as they do for this device? It’s good business? Not so fast. Dr. Paul Levy stated back in 2007 about this very procedure:
Here you have it folks — the problem facing every hospital, and especially every academic medical center. Do I spend over $1 million on a machine that has no proven incremental value for patients, so that our doctors can become adept at using it and stay up-to-date with the “state of the art”, so that I can then spend more money marketing it, and so that I can protect profitable market share against similar moves by my competitors?
No, hospitals are employing this just to keep pace. The real winner in this is Intuitive Surgical, Inc., who has been a darling of Wall Street, beating estimates in earnings with a Q2 net profit of $62.4 Million.
Why is the cost of healthcare going up while physician reimbursement goes down and hospitals go out of business?
It’s Intuitive.
God Bless America!



*This blog post was originally published at Musings of a Distractible Mind*
September 16th, 2009 by DrWes in Better Health Network, Opinion
No Comments »

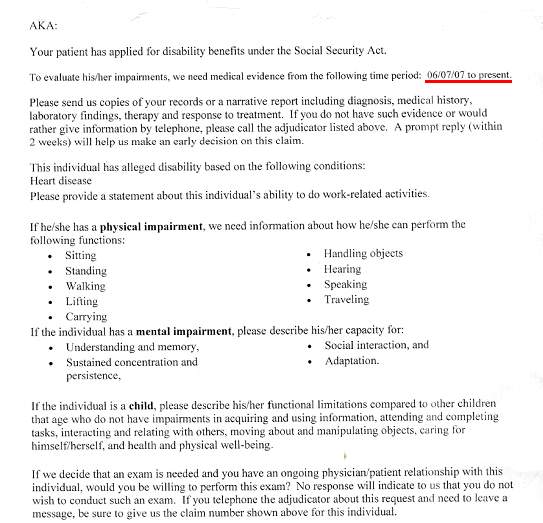
This week, like many doctors in primary care, I was sent a request by the Social Security to provide “medical evidence” that one of my patients was disabled so they could collect Social Security benefits. As part of that request, I was asked to provide evidence since June 6th, 2007, that my patient qualified for disability on the basis of “alleged” diagnosis of “Heart Disease.”
I was asked to send “copies of records or a narrative report including diagnosis, medical history, laboratory findings, treatment and response to treatment.” Beyond this, I also had to include physical and emotional impairment assessments and a functional assessment of their ability to sit, stand, walk, lift carry, handle objects, hear, speak, travel, and wash their car, view films, and eat bon bons (well, kind of).
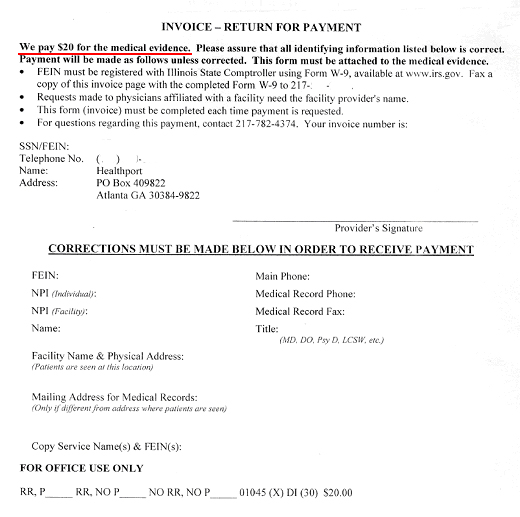
And for this copying, writing, mailing, collating what might I see from the government to compensate my time? Well, if I attach this invoice that requires a Federal Employee Identification Number filed through form W-9 available at www.irs.gov (yes, Virginia, this compensation is taxed), I might receive…
…drum roll, please…
… twenty dollars.
Now looking up the lowest paygrade of Social Security worker’s annual compensation of $29,726 and accounting for the 13 vacation days, 13 paid sick leave days, and 10 federal holidays they get paid, I estimate the least expensive Social Security employee makes a bit more than $16.50 an hour.
If we assume that the paperwork they just asked for takes about 2 hours collectively of office staff and doctor time, I think it’s clear that doctors’ payment for this service provided on behalf of our patients is substantially less than what the Social Security administration pays their own staff.
I wonder what else the government has in store for us.
-Wes
*This blog post was originally published at Dr. Wes*
September 16th, 2009 by KevinMD in Better Health Network, Health Policy, Opinion
No Comments »

by Charles W. Patterson, MD
Health care reform has long been one of my main interests and currently, it seems to be everyone else’s. The President said he thought a single-payer system would be best, but submitted a proposal he thought could be passed. The outcome is in doubt.
Actually, the single-payer system is the second best possible solution. The government would hold the money but would remain vulnerable to political manipulation, bureaucratic inefficiency.
The best system would be a well regulated “Everybody Hold Your Own Money and Pay Your Own Way System.” It would empower patients to deal directly with their caregivers without third-party interference or regulation and lead them to become sensitive to the potential benefit and the cost of their care.
This could be accomplished without taxes and without insurance premiums by a properly designed system of health care savings accounts (HCSAs). These should be funded with pre-tax money from regular automatic savings, like payroll deductions, and everyone should have one from birth. Children’s accounts should be funded by their parents. In only a couple of years, normally healthy people would save enough to stay ahead of their health care expenses. They would save the same money they now pay in insurance premiums, so once in place, the new system would cost less because no money would go to insurance company administration and profit, and unnecessary procedures and tests would decrease because people would keep the money they didn’t spend.
When any account becomes large enough to cover anticipated needs (with, say, 90 percent probability) the extra money could be rolled over into a retirement account, or children’s HCSAs. At death, a person’s HCSA could be rolled over to heir’s HCSAs, after an inheritance tax which would be used to fund HCSAs for the poor and unhealthy. Everyone would keep the money they didn’t spend, so they would not spend it unnecessarily.
Government’s role would become only regulatory. A commission might be needed to determine a fair market value for services and patented drugs, but it is likely that market forces would control these and make the mix of available services more appropriate to people’s needs.
To insure that account money was spent on effective care, and not wasted or stolen by fraud, standards of medical practice should be established with a Wikipedia-style online system to allow each licensed practitioner and researcher to propose, amend and vote on standards of practice in his or her’s field. A true consensus statement would then be available on every relevant standard of practice, which would be more up to date and represent truly effective practice, better than the opinions of a panel of “experts.”
The quality of evidence on any issue varies from one study to the next, and leaves room for differences in opinion about what is good treatment. HCSAs should be allowed to pay for all procedures which received an overwhelming vote of approval, and not for those with overwhelming disapproval. The more money in an account, the lower a procedure’s vote would need to be to have it included. The list of approved procedures would change, and its quality would improve as fast as new evidence and experience accumulated.
Regulations should also end patents for new drug which do the same thing as established drugs, as well as new preparations of established drugs. Advertising of prescription drugs should end, because it leads to unrealistic expectations and misdiagnosis. And these regulations should require saved money to be invested conservatively.
Charles W. Patterson is a psychiatrist.
*This blog post was originally published at KevinMD.com*
September 16th, 2009 by SteveSimmonsMD in Primary Care Wednesdays
No Comments »
The debate on Health Care Reform has devolved into partisan politics with each side denigrating the ideas of those they oppose instead of objectively searching for real and effective reform. In the September 4 issue of the Washington Post, an Alec MacGillis’ article “The Unwitting Birthplace of the ‘Death Panel’ Myth” shows how partisan politics brought about the destruction of a very good idea. The piece details how those on the far Right disingenuously represented a provision in the House Health Care Bill to compensate physicians for time spent counseling their patients about end-of-life decisions.
I’d like to add a physicians’ perspective to both Mr. MacGillis’s story and an important aspect of life … death. I applaud the efforts of those who tried to have this provision added to the HC Reform Bill and believe that it supported the doctor-patient relationship while trying to preserve the dignity of human life. I ask: “Are we really supposed to believe that paying physicians to talk to their patients about death will lead to the creation of ‘Death Panels’?”
If you were to collapse right now and an ambulance sped you to a hospital Emergency Room, physicians and nurses would work to save your life, exhausting all options. If you survived a prolonged effort at resuscitation this would likely be your ticket to a stay in the Intensive Care Unit (ICU) and with luck you would survive to resume your normal life as you had before. It seems simple, right?
Wrong.
A whole host of what-ifs come to mind. What if you have terminal cancer? What if you are chronically ill? What if you have already spent months in an intensive care unit and desired never to experience that again? What if you are left brain dead, to be characterized euphemistically as being in a persistent vegetative state? Would you want your body to be kept alive, cast adrift without your mind to steer it?
I could go on and never run out of possible what-if scenarios. That’s what you have your doctor for and if you haven’t talked to your primary care doctor about scenarios specific to you, then you have surrendered control of how you die to a combination of chance and the decisions of your family. Furthermore, you are transferring all responsibility for these decisions from yourself to your loved ones and that includes the guilt that comes with making hard decisions.
Here are three tools that can express your wishes and absolve your loved ones from the burden of near-impossible decisions while also allowing you to protect the dignity of your own life as you alone can truly define:
1. Living Will: A legal document which goes into effect if you can no longer speak for yourself. It will make your wishes regarding a variety of life prolonging medical treatments known to the physicians treating you. One example would include whether or not to be kept alive in a persistent vegetative state by tube feedings. It is also referred to as an advance directive.
2. DNR Order: This stands for “Do Not Resuscitate.” In the event that your heart stops beating or you stop breathing, Emergency Personnel will be required to try to ‘bring you back.’ This includes electric shocks, chest compressions, and putting a tube into your windpipe to breath for you. These invasive techniques can be life-saving but for some patients only delay death for a short period of time. Since being shocked by electricity, having someone break your ribs doing chest compressions, or having a plastic tube in your throat are all painful, one’s doctor should make clear to their patient if these efforts would be futile and a DNR order fully explained. It does not prevent you from being treated.
3. Durable Power of Attorney for Health Care: Families (usually spouses and adult children) can make health care decisions for you if you are unable to. But families tend to disagree and by assigning a power of attorney you have the chance to pick someone whose views more closely match your own or who you trust to follow your own wishes.
It takes time for a physician to adequately answer questions regarding end-of-life decisions and for most primary care doctors today, there is no time for it. I used to be scared to mention a DNR or living will to my patients, aware that doing so could translate into an hour wait for every person scheduled to see me for the rest of the day.
If primary care doctors were reimbursed for time spent discussing end-of-life decisions more people would have living wills and DNRs, and this would pay both financial and ethical dividends to our society. We would not waste so much money on people at the end of their life; and I am quite comfortable stating that to keep someone alive by artificial means when they wouldn’t have wanted it is wasteful. Ethical dividends would include protecting the dignity of human life, easing the emotional burden of loved ones in a time of crisis, and giving some control to individuals in deciding how they die — an unavoidable aspect of life that our society needs to honestly discuss and plan for. We will all die but many of us first suffer needlessly and at great expense because we didn’t plan for it ahead of time.
Until next week, I remain yours in primary care,
Steve Simmons, MD










{kind=link}
{kind=link}