July 27th, 2015 by Dr. Val Jones in Health Tips, True Stories
2 Comments »
 I met my newly admitted patient in the quiet of his private room. He was frail, elderly, and coughing up gobs of green phlegm. His nasal cannula had stepped its way across his cheek during his paroxsysms and was pointed at his right eye. Although the room was uncomfortably warm, he was shivering and asking for more blankets. I could hear his chest rattling across the room.
I met my newly admitted patient in the quiet of his private room. He was frail, elderly, and coughing up gobs of green phlegm. His nasal cannula had stepped its way across his cheek during his paroxsysms and was pointed at his right eye. Although the room was uncomfortably warm, he was shivering and asking for more blankets. I could hear his chest rattling across the room.
The young hospitalist dutifully ordered a chest X-Ray (which showed nothing of particular interest) and reported to me that the patient was fine as he was afebrile and his radiology studies were unremarkable. He would stop by and check in on him in the morning.
I shook my head in wonderment. One look at this man and you could tell he was teetering on the verge of sepsis, with a dangerous and rather nasty pneumonia on physical exam, complicated by dehydration. I started antibiotics at once, oxygen via face mask, IV fluids and drew labs to follow his white count and renal function. He perked up nicely as we averted catastrophe overnight. By the time the hospitalist arrived the next day, the patient was looking significantly better. The hospitalist left a note in the EMR about a chest cold and zipped off to see his other new consults.
Similar scenarios have played out in countless cases that I’ve encountered. Take, for example, the man whose MRI was “normal” but who had new onset hemiparesis, ataxia, and sensory loss on physical exam… The team assumed that because the MRI did not show a stroke, the patient must not have had one. He was treated for a series of dubious alternative diagnoses, became delirious on medications, and was reassessed only when a family member put her foot down about his ability to go home without being able to walk. A later MRI showed the stroke.
A woman with gastrointestinal complaints was sent to a psychiatrist for evaluation after a colonoscopy and endoscopy were normal. After further blood tests were unremarkable, she was provided counseling and an anti-depressant. A year later, a rare metastatic cancer was discovered on liver ultrasound.
Physicians have access to an ever-growing array of tests and studies, but they often forget that the results may be less sensitive or specific than their own eyes and ears. And when the two are in conflict (i.e. the patient looks terrible but the test is normal), they often default to trusting the tests.
My plea to physicians is this: Listen to your patients, trust what they are saying, then verify their complaints with your own exam, and use labs and imaging sparingly to confirm or rule out your diagnosis. Understand the limitations of each study, and do not dismiss patient complaints too easily. Keep probing and asking questions. Learn more about their concerns – open your mind to the possibility that they are on to something. Do not blame the patient because your tests aren’t picking up their problem.
And above all else – trust yourself. If a patient doesn’t look well – obey your instincts and do not walk away because the tests are “reassuring.” Cancer, strokes, and infections will get their dirty tendrils all over your patient before that follow up study catches them red handed. And by then, it could be too late.
May 8th, 2011 by Elaine Schattner, M.D. in True Stories
No Comments »

Last week I had some blood tests taken before a doctor’s appointment. I went to a commercial lab facility, one of several dozen centers for collecting specimens have opened up in otherwise-unrented Manhattan office spaces lately.
I have to say I really like getting my blood work done at this place, if and when I need blood tests. And it’s gotten better over the past few years.
First, pretty much all they do in the lab center is draw blood and collect other samples based on a doctor’s orders. So the people who work there are practiced at phlebotomy, because it’s what they do most of the time. The guy who drew my blood last week did the same a year or two ago, and he was good at it back then. He used a butterfly needle and I didn’t feel a thing.
Second, they seem organized and careful about matching specimens to patients. The man who drew my blood didn’t just confirm my name and date of birth, but he had me sign a form, upon my inspecting the labels that he immediately applied to the tubes of blood he drew from my right arm, that those were indeed my samples and that I was the patient named Elaine Schattner with that date of birth and other particulars. Read more »
*This blog post was originally published at Medical Lessons*
November 14th, 2010 by Davis Liu, M.D. in Better Health Network, News, Opinion, Research
No Comments »

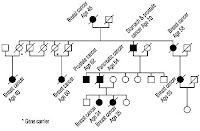 The Associated Press ran a provocatively-titled piece recently, “Family health history: ‘best kept secret’ in care”, which noted how a geneticist at the Cleveland Clinic discovered that asking about family members and their history of breast, colon, or prostate cancer was better than simply doing genetic blood testing.
The Associated Press ran a provocatively-titled piece recently, “Family health history: ‘best kept secret’ in care”, which noted how a geneticist at the Cleveland Clinic discovered that asking about family members and their history of breast, colon, or prostate cancer was better than simply doing genetic blood testing.
Surprising? Hardly. This is what all medical students are taught. Talk to the patient. Get a detailed history and physical. Lab work and imaging studies are merely tools that can help support or refute a diagnosis. They provide a piece of the puzzle, but always must be considered in the full context of a patient. They alone do not provide the truth. Read more »
*This blog post was originally published at Saving Money and Surviving the Healthcare Crisis*
November 3rd, 2010 by GarySchwitzer in Better Health Network, Health Policy, News, Opinion, Research
No Comments »

Continuing this week’s spontaneous theme (we didn’t make the claims and write the stories) of runaway enthusiasm for various screening tests by some researchers and journalists, HealthDay news service has reported on a study published in the Oct. 28 issue of the journal Nature that they say “provides new insight into the genetics of pancreatic cancer.” In the story, they let one of the researchers get away with saying, almost unchallenged:
“What’s important about this study is that it’s objective data in support of why everyone should be screened for pancreatic cancer.”
Mind you, this was a study that looked at tissue from just seven patients. The story continued with its breathless enthusiasm for the pancreatic cancer screening idea:
“In the future, new imaging techniques and blood tests will offer hope for early detection, the study noted. And just as people have a colonoscopy when they turn 50, “perhaps they should have an endoscopy of their upper gastrointestinal organs that includes an ultrasound of the pancreas,” said (the researcher).”
The very end of the story included some skepticism from Dr. Len Lichtenfeld of the American Cancer Society. Read more »
*This blog post was originally published at Gary Schwitzer's HealthNewsReview Blog*
January 3rd, 2010 by GruntDoc in Better Health Network, True Stories
No Comments »


It’s going to take a while to draw all those labs. And the patient will probably need a transfusion at the end of it.
(Reportedly the printer engaged itself in a loop and printed out blood culture label sets 25 times, so don’t panic).
*This blog post was originally published at GruntDoc*









