September 16th, 2009 by DrWes in Better Health Network, Opinion
No Comments »

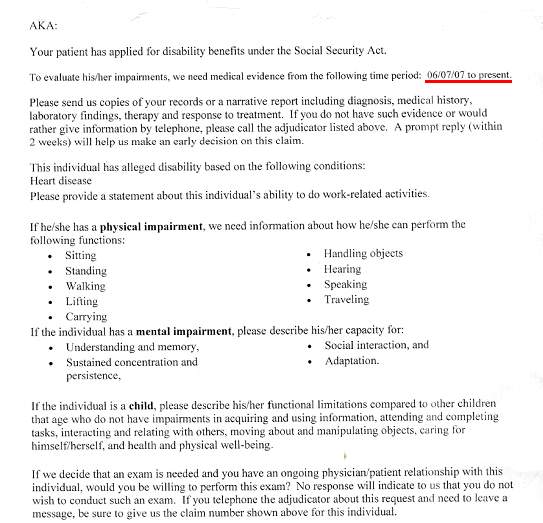
This week, like many doctors in primary care, I was sent a request by the Social Security to provide “medical evidence” that one of my patients was disabled so they could collect Social Security benefits. As part of that request, I was asked to provide evidence since June 6th, 2007, that my patient qualified for disability on the basis of “alleged” diagnosis of “Heart Disease.”
I was asked to send “copies of records or a narrative report including diagnosis, medical history, laboratory findings, treatment and response to treatment.” Beyond this, I also had to include physical and emotional impairment assessments and a functional assessment of their ability to sit, stand, walk, lift carry, handle objects, hear, speak, travel, and wash their car, view films, and eat bon bons (well, kind of).
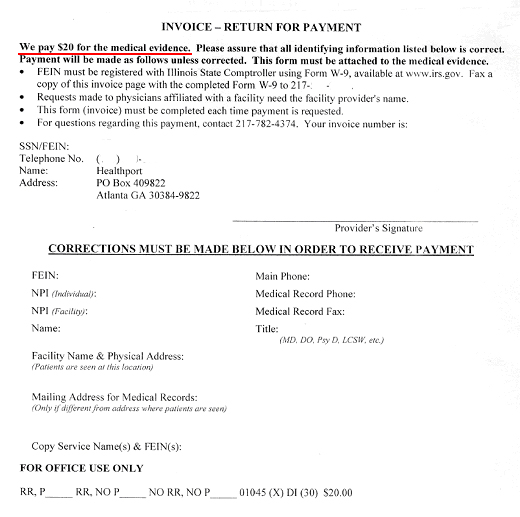
And for this copying, writing, mailing, collating what might I see from the government to compensate my time? Well, if I attach this invoice that requires a Federal Employee Identification Number filed through form W-9 available at www.irs.gov (yes, Virginia, this compensation is taxed), I might receive…
…drum roll, please…
… twenty dollars.
Now looking up the lowest paygrade of Social Security worker’s annual compensation of $29,726 and accounting for the 13 vacation days, 13 paid sick leave days, and 10 federal holidays they get paid, I estimate the least expensive Social Security employee makes a bit more than $16.50 an hour.
If we assume that the paperwork they just asked for takes about 2 hours collectively of office staff and doctor time, I think it’s clear that doctors’ payment for this service provided on behalf of our patients is substantially less than what the Social Security administration pays their own staff.
I wonder what else the government has in store for us.
-Wes
*This blog post was originally published at Dr. Wes*
September 9th, 2009 by EvanFalchukJD in Better Health Network, Health Policy
No Comments »

Newsweek tries to refute the “Five Biggest Lies In the Health Care Debate.”
But I’ve heard much bigger lies than the ones in this article.
I mean, are people really showing up angry at town hall meetings over fears that “the government will set doctor’s wages”?
Misinformation – or just plain old confusion – about our health care system is common. To try to help fix this, I offer five of the biggest, most commonly repeated misconceptions I hear regularly about the U.S. health care system.
1. Government plays a relatively small role in American health care. Government actually plays a big role. In 2007, federal, state and local governments paid for more than 46 cents of every health care dollar – more than $1 trillion. In fact, since 1980, the government has paid at least 40 cents of every dollar, and as early as 1960 – 5 years before Medicare – government paid a quarter of health care expenses. Government is a massive health care customer and has the impact one might expect such a big customer to have.
2. Health insurance companies drive the increasing cost of care in America. Not true, and here’s why: perhaps 200 million Americans don’t get their coverage from a health insurance company.
Most of these people, or a family member, work at one of the thousands of companies that self-insure (the rest are covered by government programs). What this means is those companies take the health care risk themselves, and use an insurance company mostly to handle the bills. For these companies, the cost of health care directly affects their bottom line. It’s one of the reasons employers have implemented so many programs to try to help their employees live healthier lifestyles, make sure they’re getting good care, and many others. Some data suggest it is working to control health care costs.
The exception is small groups and individuals. They have to buy health insurance, and face few, expensive options. There are many reasons for this, which I’ve blogged about extensively here. One of the most important is that there is not a truly competitive market for this kind of coverage. Still, many of these insurance companies are not-for-profit (some say as many as half of Americans with health insurance are covered by non-profit plans), and so it cannot be that profit drives the premium increases they, too, experience.
3. America has a free market in health care. Health care may be the most heavily regulated industry in America, with layers of state and federal regulation of care and insurance. For example, your doctor can only practice in the state in which he is licensed. If he wants to move to another state and be a doctor there he can’t do it unless he’s gone through a licensing process in that other state.
One of the most important reasons why the market for health insurance is so uncompetitive is that it, too, is regulated by 50 different state bodies. If an insurer wants to sell in another state, it has to go through an extensive process in order to do it, and be subject to all kinds of mandates and other requirements that make it very impractical to do so. It makes for a market that is much less dynamic than it could be.
I suspect one reason people call the U.S. system a “free market” is that rich or well-connected people can get better care than those who are less fortunate. This may be true, but this is just a reality of the human condition, not the health care system.
4. There is an Obama reform plan, and you’re either for it or against it. Much of the media – and even Chuck Norris – describe the various health care reform ideas as part of an “Obama plan” or “ObamaCare.” But other than broad outlines of what the President thinks are important principles, the President has not proposed any plan. Most of what people are talking about – including the entirety of the Newsweek article I started this post with – is the 1,017-page bill from the House Ways and Means Committee. While there are indications that the President is going to propose something concrete in the coming days, calling what is on the table Obama’s plan is more politics than reality.
5. Rising health care costs are a uniquely American problem. America’s not the only country suffering with rising health care costs. In Canada, for example, the government of British Columbia has seen its health care costs increase by 45% over the last 6 years. It’s created a budget crisis, and efforts to steadily increase the premiums it charges consumers and employers. The U.K. has actually experienced a higher rate of growth in health care costs than the U.S. over the last several years. So while it is true that the cost problem is worse in America than in in other countries, this is a matter of degree, not of kind.
I’ve heard lots of others, but these are the ones I most commonly run into.
What kinds of misconceptions have you heard?

*This blog post was originally published at See First Blog*
September 3rd, 2009 by EvanFalchukJD in Better Health Network, Health Policy
No Comments »
Bad news in the paper today: health care costs are expected to rise another 10.5% next year. It’s a serious problem that affects businesses and families across the country.
But the headlines miss something important: the rate of increase has been steadily slowing.
Are we already bending the health care cost curve?
Here is a chart of the rate of increase in health premiums for a PPO plan beneficiary from 2002-2009 (all data are from today’s Aon press release):

The data for other plan types are similar. What’s happening?
Aon’s Chief Medical Officer Paul Berger says it’s because of the variety of measures employers have taken over the last several years to implement programs to improve their employees’ health. He emphasizes there is still much more to be done.
He has a point. It’s something we have seen in our survey of major employers, and in the work that leading employers like EMC and Genzyme are doing. It’s what my company does, too. Employers are getting increasingly sophisticated at understanding what drives their health care expenses and are developing increasingly effective ways at addressing them.
So, yes, of course, we need reform of our health care system, and of course rising health care costs are a serious concern. But American employers are doing something about these problems all on their own.

*This blog post was originally published at See First Blog*
August 18th, 2009 by Emergiblog in Better Health Network, Health Policy, True Stories
2 Comments »

She didn’t eat her dinner Friday night.
By 4: 30 am Saturday, the previously healthy 65-year-old female had a fever and lower extremity weakness. A family member heard her repetitive moaning. The patient got up to void, but could barely negotiate the one step up to the hallway. As she negotiated the hallway, she staggered.
By 5:00 am she was in the ER.
*****
The patient was taken to an exam room. Vital signs were taken and it was noted that the patient’s fever was “extremely high”. The doctor came into the room and the temp was re-taken. Extremely high. The patient had no insurance and was not verbal; the doctor discussed options with the family member.
The goal: find the source of the fever and begin treatment. A CBC, Chem 14, a urinalysis, an IV and hydration would be started. No lactate level would be done; the doctor stated it would be pointless to run a test that she already knew would be elevated based on clinical presentation. Blood cultures would be drawn, but not sent immediately. As the doctor explained, they are expensive and it would take days before the test results would be back.
In this facility, payment was expected at the time of treatment and a detailed estimate was provided to the family. The low end of the estimate was the deposit.
*****
By 8:30 am Saturday, the fever was still raging; the lab tests were normal. The patient was in ice packs with a fan in an attempt to lower the fever. An IV antibiotic was initiated; hydration was on-going. An internist and a neurosurgeon were consulted as the patient was experiencing lower back pain in addition to the profound weakness. The patient was admitted.
Further tests were proposed: lumbar x-ray to rule out spondylitis and, given the patient’s age, a chest x-ray to rule out occult pneumonia. The pros and cons of each test were fully explained along with rationale and the cost.
*****
The radiographic exams were normal. A loose bowel movement that morning had been blood-tinged. The patient had been medicated for pain. A second antibiotic was started. The next step would be an abdominal ultrasound, as no obvious source for the fever had been found. The rationale for the test and the cost were discussed and the family gave the go-ahead.
The spleen. Enlarged and mottled on ultrasound. A call was made to the family to discuss needle aspiration to rule out lymphoma.
*****
Monday morning the patient’s fever was down. She was eating. She was voiding. She was still weak, still moved slowly and awkwardly. She would be discharged home on oral antibiotics with the results of her spleen aspirate pending.
*****
It’s been a week now and the patient is acting 100% normally.
The patient was my dog, a 10-year-old, 70 pound Shepherd mix. We still don’t know what nearly killed her last weekend. The spleen aspirate was abnormal, but not lymphoma. The fact that the fever responded to antibiotics (as did the weakness) leaves us with the feeling that it was an infection in such an early stage that the source was not obvious.
I realize veterinary medicine is not human medicine, and a million holes can be found in my attempt to draw a parallel between them. But a few things crossed my mind during this experience:
(a) Tests were not done just for the sake of testing or because a printed standard said they should be. This was not template medicine dictated by any outside organization or government regulations.
(b) The doctor/patient relationship was unencumbered by insurance company approvals, government regulations, billing, coding or the number of patients that had to be seen in a certain time frame.
(c) there was full transparency regarding what each test would cost.
Maybe the human health care system can take a few pointers from what the veterinary world has been doing all along.
(P.S. I just realized you can read this story from the vantage point of ME being the third-party payer standing between the vet and my dog, deciding what would be “covered” – i.e. paid for. Interesting either way….)
*This blog post was originally published at Emergiblog*
August 12th, 2009 by Gwenn Schurgin O'Keeffe, M.D. in Better Health Network
No Comments »

During a recent emergency room shift, I treated a 12 year old boy for a swimmer’s ear. During the visit, I learned he was from the South and was in the area visiting relatives before starting school in a couple weeks. It turns out he’s been battling this pain for a couple weeks and his mom is convinced it’s because of all the swimming he’s done this summer. Instead of rushing him to his own pediatrician at home, she has been “riding it out” to see if the pain resolved on it’s own.
This was true music to my ears! Most parents rush their kids to the doctor at the first sign of ear pain, even though the current recommendations are to not use antibiotics in this age group unless the pain persists or worsens past the first few days. So, if his exam were abnormal, my decision making process would be much simpler.
What wasn’t music to my ears was learning I was the second physician to see the boy that week. The grandmother took him to see her physician when she had a scheduled appointment a couple days earlier, “just for a curbside” and learned that he did in fact have “an ear infection”. No medications were given or appointment facilitated with a pediatrician or other physician. This was truly just a curbside. The family was left with no alternative but to use the ER.
The ER often ends up being our only option when visiting an area out of town, isn’t it? If staying at a hotel, many do have a cool option that provides a physician call service so a physician will come to you, as I learned a couple year’s back in Disneyland. And, some cities do have free-standing urgent-care centers that can help with these sorts of non-911 situations. But, by and large, the ER is it in most areas and for most people.
What a backwards situation! The majority of sick people have situations that do not need the ER yet find themselves having to because there are simply no other options. Think about how much time and money would have been spared for this family and the system had that first physician just seen the child as an office visit and written the same prescriptions I wrote 2 days later during the ER visit. Think about the healthcare savings to the system and personal savings to families if we had the same theoretical options to the hundreds of thousands of annual after-hours urgent care visits our system sees each year but is current seeing in the wrong setting!
In the big picture, seeing a basic sick visit after hours in the ER is like trying to crack a nut with a sledgehammer. It makes about as much sense, too. The truth is we just have no place for the after hours regular sick people, which, by the way, are the majority of people who get sick after hours, especially if their doctor is in another state!
It’s really not a shock ER wait times are so long…ERs are over loaded with patient’s just like this boy. Until we find a better system, better take along your iPod and a good book should you find yourself heading to the ER. You’ll be in very good company waiting to be seen so may as well come prepared for the wait.
*This blog post was originally published at Dr. Gwenn Is In*









{kind=link}
{kind=link}
{kind=link}