January 19th, 2011 by StevenWilkinsMPH in Better Health Network, Health Tips
2 Comments »

We’ve all been there. It often starts with some kind of recurring pain or dull ache. We don’t know what’s causing the pain or ache. During the light of day we tell ourselves that it’s nothing. But at 3:00am when the pain wakes you, worry sets in: “Maybe I have cancer or heart disease or some other life-ending ailment.” The next day you make an appointment to see your doctor.
So now you’re sitting in the exam room explaining this scenario to your doctor. Based on your previous experience, what’s the first thing your doctor would do?
A. Order a battery of tests and schedule a follow-up appointment.
B. Put you in a patient gown and conduct a thorough physical examination, including asking you detailed questions about your complaint before ordering any tests.
If you answered “A,” you have a lot of company. A recent post by Robert Centor, M.D., reminded me of yet another disturbing trend in the doctor-patient interaction. The post, entitled “Many doctors order tests rather than do a history and physical,” talks about how physicians today rely more on technology for diagnosing patients than their own “hands-on” diagnostic skills — a good patient history and physical exam, for example.
Prior to the technology revolution in medicine over the last 20 years, physician training taught doctors how to diagnose patients using with a comprehensive history and physical exam. More physicians today are practicing “test-centered medicine rather than patient-centered medicine.” Medical schools focus on teaching doctors to “click as many buttons on the computer order set as we possibly can in order to cover every life-threatening diagnosis.” The problem is that medicine is still an imperfect science, and technology is not a good substitute for an experienced, hands-on diagnostician. Read more »
*This blog post was originally published at Mind The Gap*
August 7th, 2010 by KevinMD in Better Health Network, News, Opinion, Research
No Comments »

A recent study from the Annals of Internal Medicine found that doctors often discounted a patient’s social situation when making a medical diagnosis.
Lead researcher Saul Weiner “arranged to send actors playing patients into physicians’ offices and discovered that errors occurred in 78 percent of cases when socioeconomic concerns were a significant factor.”
Evan Falchuk, commenting on the results, provides some context:
It’s hard to expect even the most gifted clinician, trying to make it through yet another week of a hundred or more patient encounters, to get these difficult decisions right. Too much of the context of a patient’s care gets lost in the endless churn of patient visits that the health care system imposes on doctors.I suspect this is enormously frustrating for doctors, although it’s worse for patients. What the researchers call a failure to “individualize care,” a patient might call “not being paid attention to.” It’s a dynamic that anyone who’s been ill has probably seen firsthand.
These findings are entirely unsurprising. Read more »
*This blog post was originally published at KevinMD.com*
June 22nd, 2010 by Davis Liu, M.D. in Better Health Network, Health Policy, News, Opinion
1 Comment »

 Boston Celtics basketball player Kendrick Perkins injured his knee during the NBA Finals against the Lakers when he landed awkwardly. Unable to weightbear, he left Game 6 not to return for the following pivotal Game 7.
Boston Celtics basketball player Kendrick Perkins injured his knee during the NBA Finals against the Lakers when he landed awkwardly. Unable to weightbear, he left Game 6 not to return for the following pivotal Game 7.
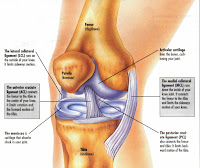
Based on his mechanism of injury and his physical examination, his trainer reported that he tore his medial collateral ligament (MCL) as well as the posterior cruciate ligament (PCL). More amazingly, this was done without the help of a MRI. Since Perkins was unable to play the final game, there was no urgent medical need to expedite the test, as regardless of the result his season was already done.
How do doctors know what’s wrong without X-ray vision or an imaging test? (Note that Perkins did get a X-ray, but X-rays generally don’t show ligament injuries.) Is it guessing? Read more »
*This blog post was originally published at Saving Money and Surviving the Healthcare Crisis*









