January 3rd, 2011 by Michael Kirsch, M.D. in Opinion, Research
1 Comment »

 The medical profession’s ability to diagnose far exceeds its ability to effectively treat the conditions discovered. Consider arthritis, Parkinson’s disease, irritable bowel syndrome, strokes, emphysema, and many cancers.
The medical profession’s ability to diagnose far exceeds its ability to effectively treat the conditions discovered. Consider arthritis, Parkinson’s disease, irritable bowel syndrome, strokes, emphysema, and many cancers.
When a physician orders a diagnostic test, ideally it should be to answer a specific question, rather than a buckshot approach. A chest X-ray is not ordered because a patient has a cough. It should be done because the test has a reasonable chance of yielding information that would change the physician’s advice. If the doctor was going to prescribe an antibiotic anyway, then why order the chest X-ray?
Physicians and patients should ask before a test is performed if the information is likely to change the medical management. In other words, is a test being ordered because physicians want to know or because we really need to know the results?
Does every patient with a heart murmur, for example, need an echocardiogram, even though this test would be easy to justify to patients and to insurance companies? If the test won’t change anything, then it costs dollars and makes no sense. Spine X-rays for acute back strains are an example of a radiologic reflex. Read more »
*This blog post was originally published at MD Whistleblower*
December 28th, 2010 by GruntDoc in Better Health Network, Opinion
1 Comment »

Via Kaiser Health News:
On a recent Friday night at the Boston Children’s Hospital ER, Dr. Fabienne Bourgeois was having difficulty treating a 17-year-old boy with a heart problem. The teen had transferred in from another hospital, where he had already had an initial work-up — including a chest X-ray and an EKG to check the heart’s electrical activity. But by the time he reached pediatrician Bourgeois, she had no access to those records so she gave him another EKG and chest X-ray. He was on multiple medications, and gave her a list of them. But his list differed from the one his mother gave doctors, neither of which matched the list his previous hospital had sent along.
This is excellent advice. Every ED has seen a patient, probably today, with “they saw me at the ER across town, but they didn’t do anything and I’m still sick.” While it makes some sense not to return to a restaurant that gave you a meal that wasn’t to your tastes, medicine is quite different.
If a patient gives me this history, I now have a blank slate, and need to essentially start at zero with them. So, I will do the correct workup to exclude the life threats based on the history and physical exam, which may be exactly the tests they had yesterday. I’m not going to assume they did the same tests, or that they were normal. It’s the standard of care at this time, and I have very, very few alternatives. Read more »
*This blog post was originally published at GruntDoc*
October 5th, 2010 by GarySchwitzer in Better Health Network, Health Policy, Health Tips, News, Opinion, Research, Video
No Comments »

We reviewed four stories on the Swedish mammography study that appeared in the journal Cancer last week. Three of the four stories gave a pretty clear indication that there were methodological concerns about the Swedish research (of the four reviewed, only HealthDay offered no such hint):
• 4th paragraph of AP story: “The new study has major limitations and cannot account for possibly big differences in the groups of women it compares.”
• 1st paragraph of LA Times blog story: “Critics charged that the study was poorly designed and potentially vastly misleading.”
• 2nd sentence of NY Times story: “Results were greeted with skepticism by some experts who say they may have overestimated the benefit.”
But none of the stories did a very complete job of explaining those potential limitations. Because of the confusion that must be occurring in the minds of women — especially those in their 40s — this is a time in which journalism must rise to the need and do a better job of evaluating evidence and helping readers make sense of what appear to be conflicting findings.
I was in Chapel Hill, North Carolina, when the study was published and had the chance to talk about it with former U.S. Preventive Services Task Force member, and a recognized thought leader on issues of prevention and especially of screening tests, Dr. Russell Harris, Professor and Director of the Health Care and Prevention Concentration of the University of North Carolina (UNC) School of Public Health. Read more »
*This blog post was originally published at Gary Schwitzer's HealthNewsReview Blog*
August 16th, 2010 by KevinMD in Better Health Network, Health Policy, Opinion
No Comments »

I’ve written previously that many doctors are finding the physical exam obsolete, and are favoring more technologically-advanced, and expensive, tests. In fact, I alluded to traditional physical exam advocates as “arguing for staying with a horse and buggy when cars are rapidly becoming available.”
In a recent piece from the New York Times, internist Danielle Ofri says we need to look past the lack of evidence supporting the physical exam. The benefits of touching the patient, and listening to his heart and lungs, cannot be quantitatively measured:
Does the physical exam serve any other purpose? The doctor-patient relationship is fundamentally different from, say, the accountant-client relationship. The laying on of hands sets medical practitioners apart from their counterparts in the business world. Despite the inroads of evidence-based medicine, M.R.I.s, angiograms and PET scanners, there is clearly something special, perhaps even healing, about touch. There is a warmth of connection that supersedes anything intellectual, and that connection goes both ways in the doctor-patient relationship.
Great point. Read more »
*This blog post was originally published at KevinMD.com*
June 22nd, 2010 by Davis Liu, M.D. in Better Health Network, Health Policy, News, Opinion
1 Comment »

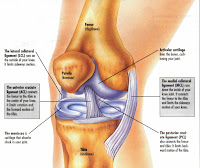 Boston Celtics basketball player Kendrick Perkins injured his knee during the NBA Finals against the Lakers when he landed awkwardly. Unable to weightbear, he left Game 6 not to return for the following pivotal Game 7.
Boston Celtics basketball player Kendrick Perkins injured his knee during the NBA Finals against the Lakers when he landed awkwardly. Unable to weightbear, he left Game 6 not to return for the following pivotal Game 7.
Based on his mechanism of injury and his physical examination, his trainer reported that he tore his medial collateral ligament (MCL) as well as the posterior cruciate ligament (PCL). More amazingly, this was done without the help of a MRI. Since Perkins was unable to play the final game, there was no urgent medical need to expedite the test, as regardless of the result his season was already done.
How do doctors know what’s wrong without X-ray vision or an imaging test? (Note that Perkins did get a X-ray, but X-rays generally don’t show ligament injuries.) Is it guessing? Read more »
*This blog post was originally published at Saving Money and Surviving the Healthcare Crisis*

 The medical profession’s ability to diagnose far exceeds its ability to effectively treat the conditions discovered. Consider arthritis, Parkinson’s disease, irritable bowel syndrome, strokes, emphysema, and many cancers.
The medical profession’s ability to diagnose far exceeds its ability to effectively treat the conditions discovered. Consider arthritis, Parkinson’s disease, irritable bowel syndrome, strokes, emphysema, and many cancers.







