January 30th, 2011 by GarySchwitzer in Health Tips, Opinion
1 Comment »

We’ve seen it before. A couple of years ago, I wrote about Roswell Park’s Prostate Club for Men offering “Prizes For Prostates” — Buffalo Sabres hockey tickets or Buffalo Bills football tickets among other awards for men who showed proof that they talked to their doctor about prostate cancer.
Now a bunch of Georgia radiotherapy centers and the Morehouse School of Medicine are among those promoting the “Georgia Prostate Cancer Coalition” and luring men in for PSA blood tests by offering them Atlanta Hawks basketball tickets.
They also promote this misleading statistic: “One in 6 men will be diagnosed with prostate cancer in their lifetime.” No explanation is given of what lifetime risk means. And no explanation is given of how many of these “cancers” are indolent and would never have harmed a man. Read more »
*This blog post was originally published at Gary Schwitzer's HealthNewsReview Blog*
January 30th, 2011 by RyanDuBosar in Opinion, Research
No Comments »

 British researchers are trying to causally link raising the thermostat to obesity prevalence.
British researchers are trying to causally link raising the thermostat to obesity prevalence.
“Domestic winter indoor temperatures” appear to be rising, the researchers wrote, as is obesity. They focused on a causal link, focusing on acute and long-term effects of being comfortable in the winter.
They write: “Reduced exposure to seasonal cold may have a dual effect on energy expenditure, both minimizing the need for physiological thermogenesis and reducing thermogenic capacity. Experimental studies show a graded association between acute mild cold and human energy expenditure over the range of temperatures relevant to indoor heating trends.”
They also look at brown adipose tissue (BAT), aka “brown fat,” the type of fat that actually consumes energy instead of stores it. We all have this fat as infants, to help us regulate our body temperatures until our bodies learn to do it on their own. The researchers suggest that “increased time spent in conditions of thermal comfort can lead to a loss of BAT and reduced thermogenic capacity.”
Determining a link “may raise possibilities for novel public health strategies to address obesity,” although I shiver to think what those strategies might entail.
*This blog post was originally published at ACP Internist*
January 29th, 2011 by Medgadget in News, Research
No Comments »

 An unexpected discovery out of Frenchay Hospital in Bristol, UK showed that deep brain stimulation (DBS) can lower blood pressure, even in cases in which drugs are unsuccessful.
An unexpected discovery out of Frenchay Hospital in Bristol, UK showed that deep brain stimulation (DBS) can lower blood pressure, even in cases in which drugs are unsuccessful.
The discovery reportedly occurred when a 55-year-old patient received a deep brain stimulator to treat his pain from central pain syndrome that developed after a stroke. At the time of the stroke, the patient was diagnosed with high blood pressure, which could not be controlled despite taking four different drugs. The deep brain stimulator was largely unsuccessful at controlling the patient’s pain, but amazingly it decreased his blood pressure enough that he could stop taking all four medications.
Researchers confirmed the effects of the deep brain stimulator by turning it on and off over a three-year period, which showed an average of a 32/12 mmHg decrease in blood pressure when the stimulator was turned on and an 18/5 mmHg increase when the device was turned off.
This breakthrough could lead to a new form of treatment for those whose hypertension cannot be controlled by drugs.
Press release from the American Academy of Neurology: Deep Brain Stimulation May Help Hard-to-Control High Blood Pressure…
Abstract in Neurology: Deep brain stimulation relieves refractory hypertension
*This blog post was originally published at Medgadget*
January 29th, 2011 by KerriSparling in Health Tips, True Stories
No Comments »

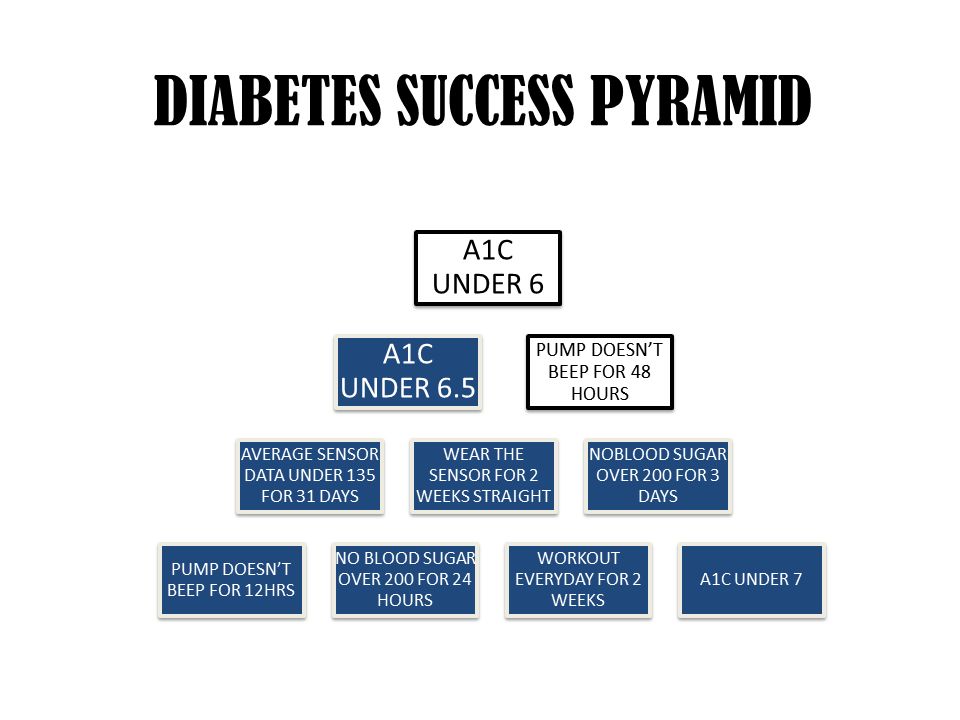
Recently, I reconnected with a long-lost local PWD (person with diabetes) named Ryan. Last time Ryan and I saw one another we were talking about diabetes goal-setting and dealing with wicked bouts of burnout. And this week I received an email from him with a brilliant idea about how to stay motivated towards setting — and reaching — diabetes-related goals.
“I’ve had this ‘pyramid’ for about three months now. Just something that I keep near my desk to keep me focused on my diabetes. After completion of the pyramid, I have no clue what I will do but some kind of celebration will be in order,” he wrote, and attached a slide to his image. And when I opened it, I was like “whoa.”
He had created a pyramid of his diabetes goals. Tangible goals — real-life goals — that are both achievable and ambitious, all at once. I thought this was so clever because it is a constant but non-threatening reminder of what diabetes goals are most top-of-mind for him. (Also, having a celebration at the end of that pyramid completion sounds like a quality idea. Perhaps a Fudgy the Whale?)
I’ve been working towards gaining better control of my diabetes (and overall health) lately, and I love the idea of something I can print out, stick to my fridge, and remain inspired by. I liked the idea of a pyramid, but I kept picturing a huge bingo hall in my mind, with a whole bunch of PWDs sitting at the tables with glucose tabs and bingo markers at the ready. But the trick wasn’t getting four in a row, it was filing the whole card.
I thought about my own personal goals and created this:

There are a few not-necessarily-diabetes-related goals on there (like “lose 6 pounds,” which is because I’m still trying to de-flump), but there are a lot of diabetes goals that aren’t unique to my particular circumstances. Since I’m trying to emerge from some diabetes burnout, my goals aren’t as tight as they were a few months ago (i.e. the slow progression from an A1C over 8 to one under 7.5). But these are real, and I’m hoping to fill the card within six months. Thanks for the fun idea, Ryan!
What would be on your bingo card?
*This blog post was originally published at Six Until Me.*
January 29th, 2011 by KevinMD in Health Policy, Opinion
No Comments »

I recently pointed to a BMJ study concluding that pay for performance doesn’t seem to motivate doctors. It has been picking up steam in major media with TIME, for instance, saying: “Money isn’t everything, even to doctors.”
So much is riding on the concept of pay for performance, that it’s hard to fathom what other options there are should it fail. And there’s mounting evidence that it will.
Dr. Aaron Carroll, a pediatrician at the University of Indiana, and regular contributor to KevinMD.com, ponders the options. First he comments on why the performance incentives in the NHS failed:
Perhaps the doctors were already improving without the program. If that’s the case, though, then you don’t need economic incentives. It’s possible the incentives were too low. But I don’t think many will propose more than a 25 percent bonus. It’s also possible that the benchmarks which define success were too low and therefore didn’t improve outcomes. There’s no scientific reason to think that the recommendations weren’t appropriate, however. More likely, it’s what I’ve said before. Changing physician behavior is hard.
So if money can’t motivate doctors, what’s next? Physicians aren’t going to like what Dr. Carroll has to say. Read more »
*This blog post was originally published at KevinMD.com*












{kind=link}