
September 21st, 2009 by Emergiblog in Better Health Network, Health Policy, Opinion
Tags: Abuse, Costs, Emergency Medicine, Finance, Fraud, Funding, Healthcare reform, Nursing, Obama, Waste
No Comments »

 Well, I lead a double life but it isn’t out dancing in formal wear!
Well, I lead a double life but it isn’t out dancing in formal wear!
“There is time for only fleeting thoughts about that dance you’ll attend during off duty hours.”
There isn’t even time for that.
Besides, who attends a dance during on duty hours?
Well, I guess the most important thing is that our hands are “soft, smooth and free from redness” because “your patients like it and your date expects it”.
Oh yeah?
The day they use a hand sanitizer thirty times in a shift and wash their hands another twenty, they can talk to me about soft hands.
********************
My husband won’t watch football with me because I tend to get hyped up and throw things at the TV when I get upset.
That explains why there were Notre Dame pom poms and a Cleveland Browns jersey at the base of the set this weekend.
I also like to talk back at the President when he is speaking on TV. Usually it’s things like “Say WHAT?” or “Give me a break!” “Get. A. Clue!” is usually a good one. This last speech, the one to Congress about health care, was no exception. My first comment came a bit into the speech when I noted a few times that “I haven’t heard a single thing I disagree with yet” and “he’s right on that point”.
I was afraid hubby was going to need smelling salts.
But I’m like, “let’s hear how he is going to pay for this…let’s hear him out”.
And then I heard it.
And then he lost me.
*****
There were two comments that I could not let go. I looked them up in the text of the speech to make sure I had heard them correctly.
“…we’ve estimated that most of this plan can be paid for by finding savings within the existing health care system a system that is currently full of waste and abuse.”
“The only thing this plan would eliminate is the hundreds of billions of dollars in waste and fraud…”
Hundreds of billions of dollars? Billions? With a capital “B”?
Waste. Abuse. Fraud.
This means that in order to pay to the proposed health care reform, we have to find enough waste, abuse and fraud to cover expenses.
*****
But I have some questions.
What is the definition of “waste”? To the extent that “waste” means inefficient bureaucratic practices that use up monetary resources, I can get on board with that.
Abuse? What kind of abuse? Using the system inefficiently, like calling an ambulance for a stubbed toe? Remember, the President is using the term “abuse” to represent a potential income stream for the new system, so it would have to encompass behaviors that spend money that should not be spent. Money is spent on patient care, so is he talking about patients abusing the system?
And then there’s fraud…
That’s a crime, folks.
Hundreds of billions of dollars in waste and fraud?
The President must think that there are an awful lot of criminals in the health care system.
So what’s my point?
*****
My point is this: funding for the new proposed health care system (see “most of this plan…”, above) is based on finding waste, abuse and fraud.
What happens when all the waste is taken out, all the abusers are stopped, the fraudsters jailed and the system needs more funding? Does that not make it imperative that we keep finding waste and abuse and fraud? Does that not mean that what constitutes waste, abuse and fraud must be constantly expanded to make up for rising costs?
This can’t be good.
I am in total agreement that our system can be streamlined, big time.
And maybe we could find enough money in waste, abuse and fraud to make it pay for itself, but I doubt it.
If we could do that, wouldn’t we have done it already with Medicaid and Medicare? The budgets for both are getting slashed on a regular basis. Drop the waste, abuse and fraud in those programs and then come back and tell me how much better their budgets are.
If we can’t do it in an existing government-provided system, how on earth do you expect us to believe it can be done on a larger scale?
*This blog post was originally published at Emergiblog*
September 20th, 2009 by Toni Brayer, M.D. in Better Health Network, Opinion
Tags: American Values, Coverage, Finance, Health Insurance, Healthcare reform, NYT
No Comments »


I read a good post from NYT about Health Care Reform and ‘American Values’ and it got me a thinkin’…just what are American Values when it comes to health care? Usually I get a little anxious when I see “American Values” in a sentence, because what usually follows is something about rugged individuality, pulling oneself up by bootstraps, getting the damn government out of our lives and those damn immigrants and welfare mothers who won’t work and want to live off others.
But I have listened to about ten thousand patients over the past 25 years, and I have a good idea of what these Americans want for health care. They are the silent majority…the people who work, study, raise their kids and seldom call into a radio talk show. They don’t have time to go to town hall meetings and shout slogans.
They range from age 17 to 101 and most of them are middle class. They come in all races…Asian, Black, White, Pacific Islander and mixes of all.
Some are wealthy enough to have multiple homes and private planes.
Some are uninsured and watch their health care spending very closely. Most were thrilled to get Medicare and I’ve never heard a complaint from a Medicare patient.
Here is my list of what these Americans think about Health Care:
- They do agree that everyone should be covered for basic health care and would pay higher taxes if they could believe that there would not be fraud and waste. (The recent banking meltdown has destroyed all confidence that government can regulate or be independent from special interests)
- They want choice of physicians and hospitals
- They are sick of insurance companies and all feel like they have been screwed in one way or another. They are shocked at how little insurance companies pay toward the doctor visit and the way those fees are discounted.
- They are technocentric and want tests, imaging, referrals and think “more is better” when it comes to health care. They think tests are cures. Because of the perverse incentives, the “more is better” philosophy benefits doctors and hospitals, but not necessarily patients.
- They fear losing insurance if they have it.
- They are confused about the current reform debate and mostly fear losing whatever coverage they now have, because they know how impossible it is to get by without any coverage at all.
There are no such thing as “American Values” because we are a diverse group of people. But we all have certain things in common. We want to be healthy. We don’t want to be screwed by anyone (big business or the government).
We want to be able to manage our own health care but we don’t want to have to decide between numerous health plans every year with pages of information that cannot be understood. We are tired of not knowing where all the $trillions really are being spent.
We want to know the price of a service up front, and we want a trusted physician to help us decide if that is how our money should be spent. We want smart, committed physicians to know us, and not hurt us.
Sounds American to me.
*This blog post was originally published at EverythingHealth*
September 17th, 2009 by Paul Auerbach, M.D. in Better Health Network, Opinion
Tags: Emergency Medicine, Learning To Practice Without Technology, Medical Practice, Outdoor Medicine, Technology, wilderness medicine
No Comments »

 This past December (2008), there was a report in Healthcare IT (Information Technology) News that got me thinking, of all things, about medical situations in outdoor wilderness environments. The substance of the report was that researchers at Vanderbilt University (I worked there in the late ’80s as Chief of the Division of Emergency Medicine) “found that physicians who receive training in a technology-rich environment, but go on to work in a less modern facility feel they can’t provide safe, efficient care.”
This past December (2008), there was a report in Healthcare IT (Information Technology) News that got me thinking, of all things, about medical situations in outdoor wilderness environments. The substance of the report was that researchers at Vanderbilt University (I worked there in the late ’80s as Chief of the Division of Emergency Medicine) “found that physicians who receive training in a technology-rich environment, but go on to work in a less modern facility feel they can’t provide safe, efficient care.”
The study related to information technology, but is probably applicable to many other modes of technology. As it was reported, the Vanderbilt study included more than 300 medical training graduates. Of those who “were working in an environment with less IT,” some 80 percent reported “feeling less able…to work efficiently, to share and communicate information, and to work effectively within the local system.” The lead investigator Kevin Johnson, MD explained that “going from being a medical student where somebody is always watching after you to a role where you could potentially make a mistake that could actually harm a patient is already hard enough.” But “when you get there and realize that the systems they have are less functional and less pervasive…there is an entirely new set of challenges.”
To all medical students, residency graduates, or anyone else who moves from a highly supervised environment to one where you are on your own, welcome to the club. The whole point of learning how to be self-sufficient is to be able to go it alone when the need arises. What is most striking about wilderness medicine is the notion that one moves to a setting that is austere and resources (people, technology, supplies, communication, etc.) are frequently limited. This can be very unsettling for experienced practitioners, and is even more so for neophytes.
We live in an age of technological imperative. Doctors train in hospitals with large, complex intensive care units. The emergency department is equipped with all the latest gadgets, and specialists are on call 24 by 7 to help out when a difficult or puzzling situation arises. That is not the case in the wilderness, on the battlefield, or out at sea. Expectations change from perfection to doing enough to get the patient to a higher level of care, or just to make it through the hour, let alone the next day.
Think about it. Take your favorite medical instrument(s) and think about how you would practice if you didn’t have access to it. Could you diagnose heart failure without a stethoscope and pulse oximeter? High altitude cerebral edema without a CT scan? Septic shock without a blood pressure monitor, central venous catheter, arterial blood gas measurements, and a battery of laboratory tests? I think the answer is “yes” if you were properly trained.
Technology is good. In fact, it is great. Patients are better off for the ability of health care professionals to apply all manner of diagnostic and interventional devices and techniques. However, I believe that at the same time we are all taught how to do things in the city, we should learn how we must sometimes do them in the country.
image courtesy of cdneverest2008.com
This post, Physicians Should Learn How To Practice Medicine With And Without Technology, was originally published on
Healthine.com by Paul Auerbach, M.D..
September 17th, 2009 by DrRich in Better Health Network, Opinion
Tags: Cardiac Electrophysiology, Cardiology, Cost, CRT, Defibrillator, Finance, Healthcare Costs, MADIT-CRT
No Comments »

When DrRich left his medical practice nearly a decade ago, he spent much of the next few years as a consultant to certain companies that make implantable defibrillators.
Most of his work was in research and development, and had next to nothing to do with defibrillators themselves, or any aspect of treating cardiac arrhythmias. Rather, DrRich was interested in developing physiologic sensors that could be deployed in implantable devices, and the algorithms that could use these sensors to predict and detect various developing medical conditions (so as to enable early intervention, and potentially prevent said medical conditions from becoming manifest). DrRich considered this work a) interesting, and b) representative of a business model that could potentially flourish within a healthcare system whose chief concern is reducing costs.
And whenever the captains of industry who signed his checks would ask him something about implantable defibrillators, usually seeking his opinion on a proposed subtle variation in some unbelievably complicated programming feature, DrRich’s reply was likely to be something like this: “Sir (or Madam) – I will be happy to study the question you pose to me, as I am working on your dime. But it greatly saddens me to see all this time, energy and talent wasted on adding yet more irrelevant features to a mature technology, in pursuit of a business model that is fundamentally broken.”
To which they would smile indulgently, hand DrRich the document describing the proposed changes, and schedule a meeting to discuss them.
The indulgent smile was in recognition of the fact that DrRich never made a secret of his disdain for the business model embraced by implantable defibrillator companies. The fact that these captains of industry put up with DrRich’s disapproval was a clear indicator that they considered it to be “quaint,” and apparently not worth taking seriously, and that the value DrRich provided in other arenas at least counterbalanced the annoyance of having him criticize their core business every chance he got.
DrRich’s disdain for the implantable defibrillator business model was based on two factors.
First, their business model relies on the artificially high prices the system will pay for their devices. DrRich has discussed this before. While these high prices are not directly the fault of the companies themselves (rather, they are fundamentally the fault of Medicare processes that distort and destroy natural market forces), these companies have now come to rely entirely on this artificial price structure, and have established all their business practices around this high-margin enterprise. The problem is that this high-price model absolutely precludes any reasonable penetration of this life-saving technology into the vast population of patients who might benefit from it. Also, because the price structure is not only artificial but arbitrary, a few simple changes in Medicare processes could abruptly destroy their business overnight.
Second, nobody is really interested in preventing sudden death. It’s difficult to sell any product when there’s no demand for that product, and there is no demand for sudden death prevention. In contrast, most other medical problems have a built-in constituency Read more »
*This blog post was originally published at The Covert Rationing Blog*
September 16th, 2009 by DrWes in Better Health Network, Opinion
Tags: Costs, Disability, Disability Determination, Government, Government-run Healthcare, Paperwork, social security, SSA, Wages
No Comments »

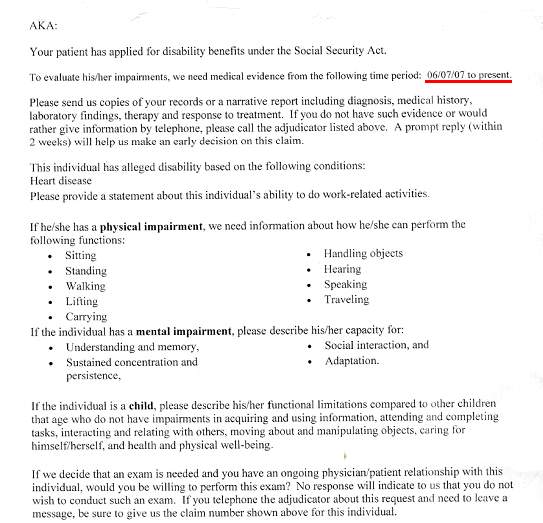
This week, like many doctors in primary care, I was sent a request by the Social Security to provide “medical evidence” that one of my patients was disabled so they could collect Social Security benefits. As part of that request, I was asked to provide evidence since June 6th, 2007, that my patient qualified for disability on the basis of “alleged” diagnosis of “Heart Disease.”
I was asked to send “copies of records or a narrative report including diagnosis, medical history, laboratory findings, treatment and response to treatment.” Beyond this, I also had to include physical and emotional impairment assessments and a functional assessment of their ability to sit, stand, walk, lift carry, handle objects, hear, speak, travel, and wash their car, view films, and eat bon bons (well, kind of).
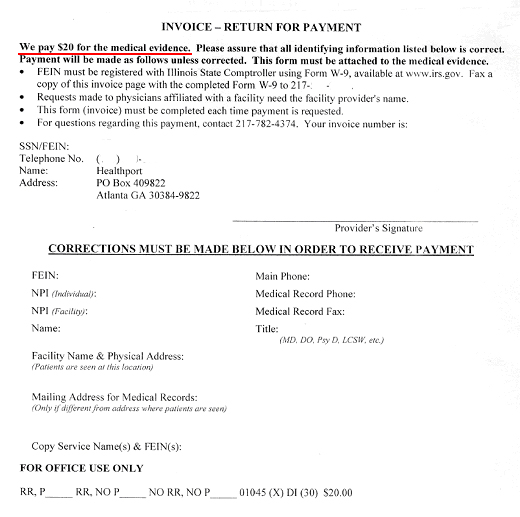
And for this copying, writing, mailing, collating what might I see from the government to compensate my time? Well, if I attach this invoice that requires a Federal Employee Identification Number filed through form W-9 available at www.irs.gov (yes, Virginia, this compensation is taxed), I might receive…
…drum roll, please…
… twenty dollars.
Now looking up the lowest paygrade of Social Security worker’s annual compensation of $29,726 and accounting for the 13 vacation days, 13 paid sick leave days, and 10 federal holidays they get paid, I estimate the least expensive Social Security employee makes a bit more than $16.50 an hour.
If we assume that the paperwork they just asked for takes about 2 hours collectively of office staff and doctor time, I think it’s clear that doctors’ payment for this service provided on behalf of our patients is substantially less than what the Social Security administration pays their own staff.
I wonder what else the government has in store for us.
-Wes
*This blog post was originally published at Dr. Wes*











{kind=link}
{kind=link}